Cocaine-induced ENT pseudo-GPA is increasingly seen in our ENT clinics. The authors of a new ENT UK guideline offer a concise overview for day-to-day recognition and management.
Use of cocaine has steadily increased in Europe since 2010 and now represents the second most common recreational drug in England, with cannabis being the front runner [1]. To increase profit margins and enhance its euphoric effect (mainly pleasure and dependency), cocaine distributers often combine (‘cut’) cocaine with numerous other compounds (‘adulterants’) with the aim to dilute the product and maximise profits. Levamisole is one of the most common adulterants used and is found in 69% of seized cocaine entering the United States [2].
Prolonged nasal insufflation of cocaine, especially if mixed with levamisole, can lead to a localised vasculitis resulting in localised sinonasal inflammation and destruction [3,4]. Little is understood about the mechanisms behind the onset and severity of the disease (e.g. dose exposure vs. individual genetic or other sensitisations) but increasing evidence is showing that an autoimmune process may contribute to its persistence, despite cessation of cocaine [5]. Agreement on terminology for this entity is still evolving, with recent evidence favouring ‘cocaine-induced ENT pseudo-granulomatosis with polyangiitis (CIEpGPA)’ [3,4]. This better encompasses the autoimmune mechanism underlaying its pathogenesis, the disease extension and generalised symptoms involving both the ear, nose and throat district, and prompts anti-inflammatory treatment with immunosuppression as well as immediate cessation of cocaine. Older terminology such as ‘cocaine-induced midline destructive lesion’ (CIMDL) falls short in recognising its pathogenesis and treatment.
"Little is understood about the mechanisms behind the onset and severity of the disease but increasing evidence is showing that an autoimmune process may contribute to its persistence, despite cessation of cocaine"
Once a rarity, CIEpGPA is becoming increasingly prevalent within ENT outpatient clinics and, therefore, early recognition is of paramount importance. No definitive diagnostic tests exist today and disease identification is based on a high suspicion arising from a combination of clinical and laboratory findings in the presence of a history of cocaine abuse.
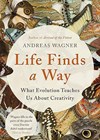
In the early stages, patients with CIEpGPA are very symptomatic, complaining of nasal pain, nasal obstruction, nasal discharge with crusting and recurrent epistaxis. As the disease advances, patients complain of severe facial pain with external nasal soft tissue destruction which ultimately affects surrounding areas including the soft palate, orbit and skull base. Nasal lesions can include small to large septal perforations, a saddle nose deformity (ranging from mild to complete nasal collapse) and significant destruction of the nasal tip and alar soft tissue (Figure 1).

Figure 1: Large septal perforation before (a) and after endoscopic decrusting
(b). Please note erosion of the inferior turbinates and of the inferior margin of the septal perforation.
Endoscopic examination typically shows the appearance of ‘vasculitis-like’ mucosa with destructive and necrotic manifestations, diffuse sinonasal crusting, bloody nasal discharge and, occasionally, bony erosion, with variable local tissue destruction extending towards (or even through) the columella, palate, lateral nasal wall, orbit or skull base (Figures 1-2).

Figure 2: MRI coronal (a) and axial (b) views of a patient with complete septal destruction,
large palate perforation and right orbital involvement following chronic cocaine use (longer than 25 years).
Laboratory findings can help in pointing towards CIEpGPA. Cocaine screening is essential, especially when cocaine abuse is not disclosed, denied or claimed as historical. A urine test, or hair sampling (where available) should be organised to confirm disease causality and avoid misdiagnosis and harmful erroneous treatments. In 70% of CIEpGPA cases, a positive pANCA is demonstrated with a PR3 preponderance, while cANCA positivity in CIEpGPA is less frequent [3]. Other tests, like urine dipsticks, chest imaging, renal function, urea and electrolytes are usually normal, which can help in the differential diagnosis with GPA. Nasal tissue biopsy is highly recommended to exclude malignancy or invasive fungal disease. Nevertheless, histology is not conclusive in the majority of cases, showing only chronic inflammation and the absence of granulomatous lesions, typical of true GPA.
The management of CIEpGPA does require rheumatology multidisciplinary team (MDT) input. It is important to nurture this rheumatology MDT approach with the aim to establish a joint ENT / vasculitis MDT within your hospital trust. The patient must stop cocaine use and, unless this is achieved, immunosuppressive treatment will not commence. Topical nasal treatments, including nasal douches and antibiotic ointments, are required to control sinonasal symptoms and infections. Under rheumatology care, a trial of systemic glucocorticoids will typically be the first line of treatment, followed by escalation to other immunosuppressants depending on disease response. Early surgery (apart from a diagnostic biopsy) is not recommended. Surgical procedures aimed to restore the nasal airway or sinus ventilation should be avoided during the active phase as these have a high risk of failure with local complications (i.e. bleeding, scarring, infections and poor healing).
Surgical reconstruction is not recommended until all clinical and biochemical signs of active inflammatory disease have remitted for a period of 12–18 months of remission. Importantly, the final decision to perform reconstruction is made jointly by the vasculitis MDT so as to confirm remission/control of the disease and minimise the risks of potential postoperative complications.This window allows enough time for the local inflammation to settle down and improve nasal tissue vascular supply. This is also a good timeframe which permits the monitoring of potential early relapse in addicts. Patients must also be warned of poor surgical outcomes due to impaired healing and lower elasticity of local tissues, as well as the potential of reactivating the vasculitis process.
CIEpGPA subjects are severely affected psychologically, compounded by the stigma of facial deformity, and this negatively impacts on quality of life and social functioning. Psychological and mental health support within the community is vital but often lacking, hence their dependence on ENT secondary care provision remains the only option available to get them through this ordeal.
Below is an extract from a CIEpGPA patient who wanted to share their experience, as well as express their gratitude for the care they received. This patient advocate is also very keen to raise public awareness regarding the long-term effects of cocaine use. Importantly this reminds us as doctors to support our patients, despite their past choices, and try to help them in their journey.
“As a patient since 2017, I have faced a challenging yet transformative journey to recovery both physically and emotionally. Receiving the appropriate referral felt like a lifeline, not only enabling my recovery but also helping me to escape a world I never intended to be part of. Although I was aware that my cocaine use was causing the pain in my nose, I sincerely had no understanding of the biological effects that it was having on me. This meant that there was a substantial amount of time where I was continuing to use, unaware of the reality that my septum was eroding by the second from tissue necrosis. The longer a patient remains unaware of the severity of their condition, the further they may drift from abstinence which can deepen their addiction, heighten feelings of loneliness and increase the risk of suicide. While every patient’s experience and response are inherently subjective, I must express that the approach I received from my physician provided me the strength I needed to change my life. Knowing I was in a safe environment for the first time in years was a light at the end of the tunnel. Having a sincere and empathic approach to cases such as mine can completely disarm a patient especially when coming from an environment of fear and toxicity. No matter how lost or broken you may feel at any given time, the right people can always piece you back together again.”
LJK – patient diagnosed with CIEpGPA and previous cocaine user for 10 years.
References
1. Office for National Statistics O. Drug misuse in England and Wales: year ending June 2022.
https://www.ons.gov.uk/peoplepopulationandcommunity/
crimeandjustice/articles/drugmisuseinenglandandwales/
yearendingjune2022
2. Centers for Disease Control and Prevention. Agranulocytosis associated with cocaine use - four States, March 2008-November 2009. MMWR Morb Mortal Wkly Rep 2009;58(49):1381–5.
3. Pendolino AL, Benshetrit G, Navaratnam AV, et al. The role of ANCA in the management of cocaine-induced midline destructive lesions or ENT pseudo-granulomatosis with polyangiitis: a London multicentre case series. Laryngoscope 2023;134(6):2609–16.
4. Andrews P, Barnes M, Sharp H, et al. Cocaine Induced ENT pseudo-GPA (CIE pGPA). British Society of Facial Plastic Surgery and British Rhinology Society Guidelines.
https://www.entuk.org/resources/204/
cocaine_induced_ent_pseudogpa_cie_pgpa/
5. Swift A, Andrews P. Granulomatous Disease, Vasculitides and the Cocaine nose. In: Swift A, Carrie S, de Souza C, (Eds.). Contemporary Rhinology: Science and Practice. Springer;2023:593–607.
[All links last accessed February 2025]
Declaration of competing interests: None declared.